East Brunswick Endoscopy Center,Inc

Faqs
FREQUENTLY ASKED QUESTIONS
The practicing physicians at East Brunswick Endoscopy Center have provided this page to provide information to Frequently Asked Questions. If you have a question that is not listed here, please give us a call.
The practicing physicians at East Brunswick Endoscopy Center have provided this page to provide information to Frequently Asked Questions. If you have a question that is not listed here, please give us a call.
What is a colonoscopy?
A colonoscopy is the direct examination of the colon (large intestine) using a slender, flexible computerized instrument.
Is the procedure painful?
Since every colonoscopy in our practice is performed after the administration of anesthesia, the procedure is virtually painless.
I want to schedule a colonoscopy, why do I need an office visit first?
Prior to colonoscopy, we must meet with you to review your medical history, family history, and to examine you. This will also be an opportunity to explain the procedure in detail, discuss the preparatory measures that are required, and answer your questions about the examination. This is a compulsory visit in our practice prior to any endoscopic procedure.
How long does the procedure last?
Between 30 and 45 minutes. Typically, a colonoscopy lasts about twenty (20) minutes. For removal of polyps or biopsies add 5-10 minutes to the procedure. .
How long will I be at the center?
Approximately 1-1/2 hours.
Are there any symptoms I may experience after the procedure?
You may experience bloating and/or gas. You may also have some abdominal cramping. On rare occasions, you may see red marks on your abdomen caused by the hands of the assistant if external pressure is applied to help guide the scope during insertion.
How I can prevent colon cancer?
INTRODUCTION:
In 2005, an estimated 140,000 Americans will be diagnosed with colorectal cancer (CRC) and about 58,000 will die from this disease. Cancers of the lung and bronchus, breast, and colon and rectum are expected to account for 51% of all cancer deaths this year. However, nearly every case of sporadic colon cancer could be prevented if every American were to undergo periodic total colonic evaluation starting at age 50. About 5.6% of Americans will develop colorectal cancer at some point throughout their lives. When colorectal cancer is diagnosed at an early stage, five-year survival is 90%.
WHO IS AT RISK?
Epidemiology:
The incidence of CRC is similar in both men and women. CRC is the second leading cause of cancer deaths in developed countries, behind lung carcinoma. It is the fourth most common carcinoma in the U.S. and accounts for 13% of all cancers. It is the third behind lung and breast cancer as a cause of cancer deaths in women.
Risk factors:
The risk factors for developing CRC are family history of colorectal carcinoma or polyps, or personal history of colon carcinoma, polyps, or inflammatory bowel disease.
SCREENING GUIDELINES:
CRC is a very preventable disease as almost all CRCs arise from premalignant polyps and if these are removed endoscopically CRC will not occur.
Recommendations for CRC Screening in people at average risk:
These are asymptomatic patients who are 50 or older with no known risk factors. The screening colonoscopy can be offered every five-ten years, as few polyps will arise and progress to advanced cancer in less time in patients with no specific risk factors. The obvious advantages are that the entire colon can be visualized and any polyps or cancers can be removed or biopsied at the time of the exam. Between 70-80% of all CRCs occur among patients at average risk. Incidentally, as of July 2001 traditional Medicare reimburses physicians for performing a screening colonoscopy in "average risk" patients. A colonoscopy is covered if the patient has not had a prior colonoscopy or flexible sigmoidoscopy within the past 10 and 4 years, respectively. The New Jersey legislature has mandated health insurances pay for screening colonoscopy in everyone 50 years and older.
Recommendations for those at increased risk for CRC:
For those with a sibling, parent, or child who have had CRC or an adenomatous polyp, the recommendations are the same options as an average risk individual, but beginning at age 40.
SUMMARY STATEMENT:
Colon cancer mortality rates have declined over the past 16 years. It is imperative that practitioners continue to make strides at screening patients for detection of polyps prior to their evolution into malignancy. Mammograms, PAP smears, and colon cancer screening should be equally considered when evaluating patients in the office. Large scale screening studies have proven that screening is cost effective and save lives
In 2005, an estimated 140,000 Americans will be diagnosed with colorectal cancer (CRC) and about 58,000 will die from this disease. Cancers of the lung and bronchus, breast, and colon and rectum are expected to account for 51% of all cancer deaths this year. However, nearly every case of sporadic colon cancer could be prevented if every American were to undergo periodic total colonic evaluation starting at age 50. About 5.6% of Americans will develop colorectal cancer at some point throughout their lives. When colorectal cancer is diagnosed at an early stage, five-year survival is 90%.
WHO IS AT RISK?
Epidemiology:
The incidence of CRC is similar in both men and women. CRC is the second leading cause of cancer deaths in developed countries, behind lung carcinoma. It is the fourth most common carcinoma in the U.S. and accounts for 13% of all cancers. It is the third behind lung and breast cancer as a cause of cancer deaths in women.
Risk factors:
The risk factors for developing CRC are family history of colorectal carcinoma or polyps, or personal history of colon carcinoma, polyps, or inflammatory bowel disease.
SCREENING GUIDELINES:
CRC is a very preventable disease as almost all CRCs arise from premalignant polyps and if these are removed endoscopically CRC will not occur.
Recommendations for CRC Screening in people at average risk:
These are asymptomatic patients who are 50 or older with no known risk factors. The screening colonoscopy can be offered every five-ten years, as few polyps will arise and progress to advanced cancer in less time in patients with no specific risk factors. The obvious advantages are that the entire colon can be visualized and any polyps or cancers can be removed or biopsied at the time of the exam. Between 70-80% of all CRCs occur among patients at average risk. Incidentally, as of July 2001 traditional Medicare reimburses physicians for performing a screening colonoscopy in "average risk" patients. A colonoscopy is covered if the patient has not had a prior colonoscopy or flexible sigmoidoscopy within the past 10 and 4 years, respectively. The New Jersey legislature has mandated health insurances pay for screening colonoscopy in everyone 50 years and older.
Recommendations for those at increased risk for CRC:
For those with a sibling, parent, or child who have had CRC or an adenomatous polyp, the recommendations are the same options as an average risk individual, but beginning at age 40.
SUMMARY STATEMENT:
Colon cancer mortality rates have declined over the past 16 years. It is imperative that practitioners continue to make strides at screening patients for detection of polyps prior to their evolution into malignancy. Mammograms, PAP smears, and colon cancer screening should be equally considered when evaluating patients in the office. Large scale screening studies have proven that screening is cost effective and save lives
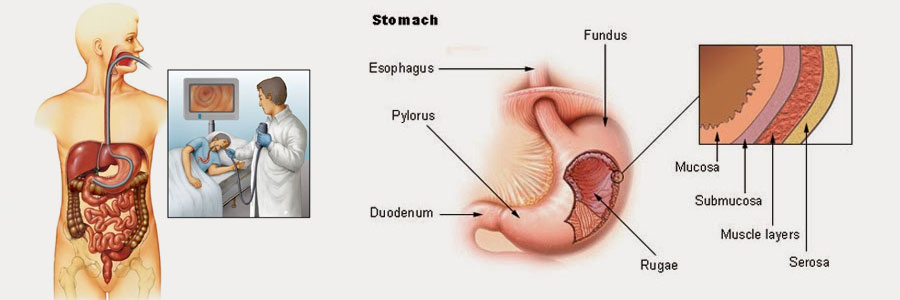
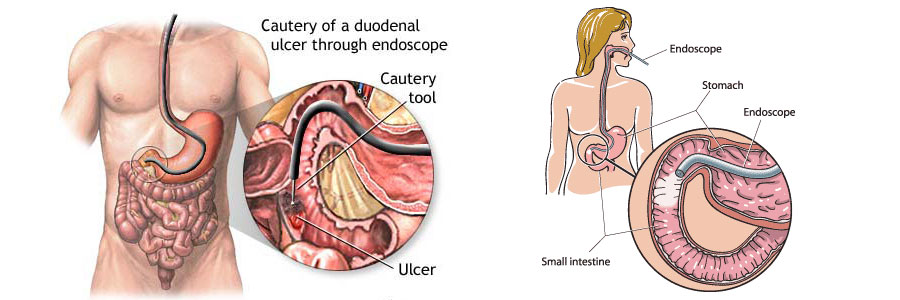
Gastroscopy

INTRODUCTION - An upper endoscopy is a procedure that allows a physician to examine the upper part of the gastrointestinal (GI) system,
Colonoscopy

INTRODUCTION - A colonoscopy is an examination of the lower part of the gastrointestinal tract, which is called the colon or large intestine (bowel).